John Stuart Mill was among the foremost liberal thinkers of modern times who wrote extensively…
Our Common Right to Health Gabriele Koehler
Acute deaths, chronic deaths
The COVID19 pandemic is frightening. The staggering number of deaths in just a few months is numbing our minds and breaking our hearts.
Medical disasters such as the current covid-19 pandemic, or natural disasters such as hurricanes, tsunamis, floods, droughts, earthquakes, or man-made disasters such as nuclear power plant implosions affect a large number of people in one incident. They are acute. They are distressing. They ought to not be happening.
At the same time, despite the enormous morbidity and mortality of the Covid19 virus, year upon year, chronic medical disasters affect far larger numbers people on this planet. But that silent catastrophe is barely mediatised – although the statistics are at our fingertips, thanks to national health observatories and the annual compilations of UN agencies such as the WHO. My guess is that is because it is more difficult to depict their impact and also because the majority of those who perish in chronic disasters don’t have a voice.
Some global numbers for our attention:
In terms of preventable premature deaths, in 2015, around 303 000 women died from causes related to giving birth (WHO 2018: 4). Every year, five and a half million children under 5 years die, either because of birth-or post-delivery complications, or because of acute respiratory infections, diarrhoea and malaria (WHO 2018: 5); the “underlying condition” often being severe malnutrition. An estimated 1.7 million persons succumbed to TB in 2016 (WHO 2018: 5). Unsafe drinking water, unsafe sanitation and a lack of hygiene led to an estimated 870 000 deaths (2016) (WHO 2018: 10).
Deaths due to public policy choices are high too. Our abuse of our planet causes preventable deaths: WHO estimates that outdoor air pollution in cities and rural areas caused 4.2 million deaths worldwide (2016) (WHO 2018: 10). Road traffic incidents killed 1.25 million people in 2013 (WHO 2018: 7), due to poor roads and lack of protective gear such as helmets.
Wars too are deadly. Of course, they could be prevented. Approximately 180 000 people were killed in wars and conflicts in 2016, with the toll steadily rising compared to preceding years (WHO 2018: 8). As a result of conflict, and – as is increasingly acknowledged, as a result of climate change effects – 70 million people are now forcibly displaced (UNHCR 2020), living in makeshift accommodation without the handwashing, physical distancing and distance-learning opportunities currently advised so vociferously.
Almost all of these deaths from chronic causes and structural health system deficiencies are premature, and preventable. And they are unequally distributed. They are concentrated in low-income countries, and in low-income households. They predominately affect disadvantaged communities – persons systematically excluded from health services because of their gender, ethnicity, caste, language, culture, faith, heir location or status as migrants and refugees, or because of their sexual identity (UNDP 2019). Or because they are children – in many patriarchal communities: girl children — or older people who are considered expendable.
My first point then is that premature, preventable deaths have both the acute and terrifying face of the current Covid-19 pandemic, but also the quiet, continuous, chronic violence of these annual huge death burdens. In terms of numbers, then, the high death toll of the Covid-19 is not “unprecedented”.”
Deaths and health systems
My second point is that many of the anticipated deaths from Covid-19 will be attributable to failings of the health system – the curve needs to be flattened because the capacity line for the health care interventions needed is far too low in every country. As some commentators have been saying, it is not just about stretching the incidence of cases, but also about lifting the line: of raising the capacity of public health systems and of provisions for catastrophes such as pandemics.
The acute medical disaster of Covid-19 is in some ways akin to the impacts of an earthquake –earthquake shocks and aftershocks pulverise buildings and infrastructure that were not compliant to security regulations, crushing and suffocating people caught inside. But not just the acute earthquake of this pandemic, also the quiet, chronic violence of “everyday” deaths needs to be addressed: health systems need to be strengthened dramatically on every level, for every health challenge and for every person.
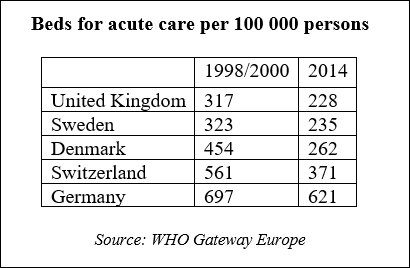
As Isabel Ortiz and Thomas Stubbs (2020) have pointed out in a radical piece, the weakness of all our health systems is ultimately due to the ideology of austerity and neoliberalism which has eaten into policy makers decisions for the past three decades. For the UK, Watkins et al (2017; UCL 2017) have shown this equally drastically, in an academic paper published already three years ago. One direct effect of this ideology has been the continuous downsizing of health system capacity. Merely looking at wealthy Europe with its welfare states, and their capacity to deal with a pandemic with exponential transmission rates, we see for example that the number of acute care hospital beds have been reduced in every country. So, the current pandemic will indeed quickly outstrip capacity – and of course acute care beds are just superficial proxies for such care which is delivered by physicians, nurses, as well as administrative, cleaning, transportation staff and many others. This is despite warnings since 2005! from the UN’s United Nations System Influenza Coordination (UNSIC) unit to globally ramp up pandemic prevention and response capacity.
Of course, the number of acute care beds doesn’t reflect the quality of a health system. Community-based settings are much more accessible, and, if properly-resourced and well-managed, can be more equitable – if on-the-ground processes of social exclusion are overcome. They are generally more efficient in preventing maternal and child mortality, or
in treating infectious diseases. Outside the formal health care system, the responsibility for care is shouldered largely by women and girls whom all societies rely on to do their care work (UN Women 2018). Here too, we need structural change, as outlined in an inspiring manifesto drafted by a global coalition of feminists from over 200 organizations (Women’s Rights Caucus. 2020).
Health systems and the right to health
Just a few years ago, the global community – that is the 193 member states of the United Nations – committed to universal health care and decided on the policies necessary to achieve that goal. There is even an acronym that many policy makers have – notionally – adopted: “UHC”. It is goal 3 of the much-cited Sustainable Development Goals (United Nations 2015). Admittedly, the vison is modest: to achieve the right to health only in a decade from now, by 2030. This is timid, given that it has been promised since 1948 in the Universal Declaration of Human Rights, and it is timid in light of global wealth of capital and of knowledge which could deliver UHC and SDG 3 immediately, if politics so decided.
As we tremulously open the newscasts or our inboxes each day to read of the ever increasing numbers of the Covid-19 victims, we need to “instrumentalise” this pandemic for the SDG commitments: stop all preventable premature deaths, be they from acute pandemics or from chronic conditions, build equitable health systems for all everywhere. We can use the 2030 Agenda to frame the polices we need.
PS – Reminder:
The SDGs commit: to universal health coverage (UHC) with equitable access to health services; to social protection to prevent deepening poverty in crises and to guarantee a decent standard of living; and to decent work – secure, safe jobs, paid properly and insured; to gender equality and recognising women’s unpaid work as they care for others; and most of all, to the promise that all are equal.
Sources:
- Isabel Ortiz and Thomas Stubbs. 2020. Fighting Coronavirus: It’s Time to Invest in Universal Public Health. Inter Press Service.
http://www.ipsnews.net/2020/03/fighting-coronavirus-time-invest-universal-public-health/ - UCL 2017. Austerity linked to 120,000 extra deaths in England Effects of health and social care spending constraints on mortality in England: a time trend analysis.
https://www.ucl.ac.uk/news/2017/nov/austerity-linked-120000-extra-deaths-england - UNDP 2019. Human Development Report 2019. Beyond income, beyond averages, beyond today: Inequalities in Human Development in the 21st Century. New York: United Nations.
http://hdr.undp.org/sites/default/files/hdr2019.pdf - UNHCR 2020. Figures at a glance.
https://www.unhcr.org/figures-at-a-glance.html - United Nations 2015. Transforming our world: the 2030 Agenda for Sustainable Development. Resolution adopted by the General Assembly on 25 September 2015. A/RES/70/1. New York: United Nations.
- UN Women 2018. Turning Promises into Action: gender equality in the 2030 Agenda for Sustainable Development. New York: United Nations.
http://www.unwomen.org/en/digital-library/publications/2018/2/gender-equality-in-the-2030-agenda-for-sustainable-development-2018#view. - Watkins J, Wulaningsih W, Da Zhou C, et al. Effects of health and social care spending constraints on mortality in England: a time trend analysis. BMJ Open 2017;7:e017722. doi: 10.1136/bmjopen-2017-017722.
https://bmjopen.bmj.com/content/7/11/e017722 - WHO 2018. World Health Statistics. Monitoring health for the SDGs.
https://apps.who.int/iris/bitstream/handle/10665/272596/9789241565585-eng.pdf?ua=1 - WHO Gateway Europe. Acute care hospital beds per 100 000.
https://gateway.euro.who.int/en/indicators/hfa_478-5060-acute-care-hospital-beds-per-100-000/visualizations/ - Women’s Rights Caucus. 2020. Feminist declaration on the occasion of the twenty-fifth anniversary of the Fourth World Conference on Women*.
https://iwhc.org/wp-content/uploads/2020/03/Beijing-25-Feminist-declaration.pdf
